| Home |
|
|
 |

| Know Dr. Patta Radhakrishna | About Surgical Gastroenterology | Appointment Schedule & Events |
Fix an Appointment | Contact Us |
|
Home » Gall Bladder and Biliary Tract Surgery
Gall Bladder and Biliary Tract Surgery What is Gall bladder and biliary tract
surgery? Usually asymptomatic, stone in gall bladder is an extremely common disorder found in people. Due to temporary obstruction of the cystic duct with a gallstone, some people suffer biliary colic, an intermittent and acute pain in the epigastrium or right upper quadrant, and at times between the scapula. The risk of inflammation in gallbladder is there if the cystic duct obstruction persists and due to this, the patient develops cholecystitis which is an acute inflammation and infection of the gallbladder. Signs and Symptoms
Majority of patients with gallstones are asymptomatic. Unlike asymptomatic, symptomatic gallstones typically grow with right upper quadrant abdominal pain. The condition is accompanied by nausea and vomiting. The pain may abate over several hours (biliary colic) and is quite severe. It may also progress to cholecystitis, with persistent pain and fever. On examination, there is pain to palpation in the right upper quadrant (Murphy's sign). Diagnosis Right upper quadrant ultrasound is the best choice for imaging study. In the ultrasound, the presence of cholecystitis shows the presence of gallstones, a thickened gallbladder wall and pericholecystic fluid. Endoscopic ultrasound is the option for the patients with symptomatic gallstones and a negative ultrasound examination. Further, a hydroxy iminodiacetic acid (HIDA) scan is useful to confirm the suspicion of cholecystitis. Concentrated radionuclide material present in liver is excreted into the bile but does not fill the gallbladder due to cystic duct obstruction. Summary: Acute Cholecystitis
Treatment Cholecystectomy is the primary treatment for symptomatic gallstone disease in which gall bladder surgery is required. Warranty of prophylactic cholecystectomy is not there for silent gallstones. In the world, most of the cholecystectomies are done laparoscopically. For a patient with an acute episode that resolves with a visit to a surgeon within a few weeks and elective cholecystectomy should be considered. Urgent care is required for those patients who have persistent right upper quadrant tenderness and develop fever or an elevated white blood cell count. In up to 10% of cases, acute cholecystitis can be accompanied with common bile duct stones. Endoscopy method after cholecystectomy is required for removing the stones. Another method is surgical that is done at the time of laparoscopic or open cholecystectomy.
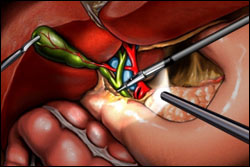
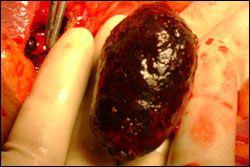
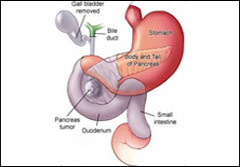
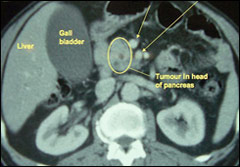
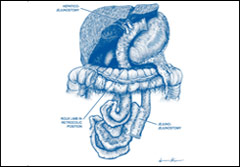
Some patients with good risk who undergo elective laparoscopic cholecystectomy are sent home within 24 hours, whereas patients who undergo open cholecystectomy may require several days of hospitalization. 95% of patients experience relief from pain after cholecystectomy. The remaining patients probably had symptoms not related to gallbladder disease before surgery. The primary treatment for symptomatic gallstone disease is cholecystectomy. Prophylactic cholecystectomy for silent gallstones is not warranted. 3 Most cholecystectomies in the world are done laparoscopically. A patient with an acute episode that resolves should see a surgeon within a few weeks and elective cholecystectomy should be considered. Patients who have persistent right upper quadrant tenderness and develop fever or an elevated white blood cell count should be seen more urgently. Pancreatic SurgeryPancreaticoduodenectomy (Whipple Procedure) This procedure is the treatment for the cancer of pancreatic head and ampulla. Also known as a Whipple procedure, in pancreaticoduodenectomy, pancreas head grown due to a tumor in the pancreas or bile duct, or pancreatitis is removed. If a tumor exists in the head of the pancreas, it becomes necessary to remove the pancreatic head, gall-bladder, duodenum and a portion of bile duct. In some cases, a part of the stomach is also removed. To ensure flow of bile and enzymes into the intestines, the end of a patient's bile duct and the remaining pancreas are connected to the small bowel. A distal pancreatectomy is indicated for tumors in the body and tail of the pancreas in which removal of neoplasms is done. Surgeons attempt to preserve the spleen with both laparoscopic and open distal pancreatectomy procedures. Drainage Procedures
Procedures to improve ductal drainage include: Longitudinal Pancreaticojejunostomy (Puestow Procedure) The pancreatic duct is attached to the small bowel after it is opened from the tail to the head of the pancreas. Distal Pancreaticojejunostomy (Du Val Procedure) The division of the pancreas is done transversely at the neck, and the body and tail are drained through an attachment to the small bowel. Sphincteroplasty In case of unsuccessful endoscopic sphincterotomy, surgical sphincteroplasty may be required of the minor or major papilla. |
||